
Treating the whole body: The case for lentiviral gene therapy’s head-to-toe reach
We hear it regularly from patients and caregivers: There’s an urgent need for therapies that can treat the whole body to address the full range of symptoms in diseases that manifest in both the central nervous system (CNS) and peripheral tissues.
Biologically, that’s a tall order. The brain is protected by an intricate blood-brain barrier designed to permit the entry of vital nutrients and other essential molecules while blocking other traffic, including circulating pathogens. This barrier is critical to our well-being in normal circumstances, but its powerful drug-exclusion properties makes it highly challenging to develop therapeutics that can treat the whole body.
This challenge has spurred a great deal of innovation. A recent review in Nature Reviews Drug Discovery walked through several technologies in development to deliver therapeutics across the blood-brain barrier, including focused ultrasound to open small breaches in the protective tissue, nanoparticle-based delivery systems and receptor-mediated transcytosis, which harnesses antibodies that bind to receptors in the blood-brain barrier to shuttle therapeutics into the CNS.
These technologies are exciting and in the future may offer new avenues for achieving whole-body treatment. However, the review article gave short shrift to a modality that has already been validated in the clinic for certain indications – and approved by regulatory authorities.
I’m talking about ex vivo lentiviral gene therapy.
This approach starts with the patient’s own hematopoietic stem cells, which are modified to carry a therapeutic gene. When the genetically modified cells are infused back into the patient, they’re expected to engraft in the bone marrow to form all the different cell types of the blood, including monocytes, some of which enter the brain where they become microglia/microglia-like cells — each of these trillions of daughter cells, carrying the therapeutic gene. To enable engraftment, patients typically undergo conditioning before their infusion. The conditioning agent most widely used in lentiviral gene therapy, busulfan, has the ability to cross the blood-brain barrier and clear space in the CNS for the genetically modified cells.
Visualizing lentiviral gene therapy’s impact in the brain
At this point, you may be wondering: How do we know that lentiviral gene therapy can affect both the body and the brain? Is there data supporting the theory that those genetically modified cells can access the CNS?
As of February 2020, there is.
That’s the publication date of a seminal study led by Nicole Wolf, M.D., Ph.D., at the Medical Center associated with the Vrije Universiteit in Amsterdam. Her team investigated the effects of donor hematopoietic stem cell transplantation on the brain tissue of two young patients with the lysosomal disorder, metachromatic leukodystrophy (MLD). Tragically, young children affected with MLD rapidly lose the ability not only to walk and talk, but to interact in any way with the world around them. In this case, unfortunately, despite the transplant, the disease progressed rapidly in both children, and both passed away. The parents gave consent for their tissue to be studied to further science.
Dr. Wolf’s findings are remarkable. For the first time in humans, she identified normal widespread distribution of donor-derived genetically modified microglia-like cells throughout the patients’ brains. What’s more, these donor cells were expressing the lysosomal enzyme arylsulfatase A (ASA) – the expected finding since the donor cells were normal. People with MLD cannot produce functional ASA due to a genetic mutation. The goal of donor HSC transplantation is to supply patients with healthy cells that contain a corrected version of the gene, and therefore produce normal functioning enzyme. After a round of conditioning with busulfan, the healthy donor cells were infused into the patients’ bodies intravenously. Daughter cells crossed the blood-brain barrier and established themselves throughout the CNS. And Dr. Wolf found that once in the brain, they continued to express functional ASA.
Look at this figure from her paper below. On the left, you see brain tissue of a young MLD patient who did not receive an HSC transplant. On the right, you see tissue from a patient who did receive the donor HSC transplant. The dark dots represent cells that are expressing the ASA enzyme. As you can see, the transplant of healthy donor cells resulted in expression of functional enzyme throughout the brain. That’s important because we and others in the field believe that restoring function to microglia-like cells and/or bathing tissue in functional enzyme 24/7 can prevent, halt or even reverse disease progression.
Allogeneic HSC Transplantation (HSCT)
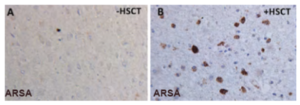
Wolf, Ann. Clin. Trans. Neuro. 2020
While the two patients that Dr. Wolf studied did not benefit in the way we would have hoped from the donor stem cell transplant, in part because supra-physiological levels of functional enzyme are required for such a therapy to work in MLD, her study demonstrates that HSC transplants can enable patients to begin producing functional enzyme that they could never before produce.
Ex vivo lentiviral gene therapy aims to deliver those benefits even more directly. With HSC treatments of the type Dr. Wolf described, stem cells from a healthy individual are transplanted into the patient. It’s often hard to find an appropriate donor — a good donor match is always hard to find, and even then there remains a high risk of graft versus host disease which often leads to serious complications. Ex vivo lentiviral gene therapy avoids those issues because it uses cells from the patient’s own bone marrow – modified so they contain a therapeutic gene that expresses the functional enzyme the patient needs for healthy cellular function.
How do we know this can work? A number of companies have produced strong data, from multiple clinical trials across multiple indications. In some cases, the benefits could rightly be described as transformational.
In December, for instance, Orchard Therapeutics received market authorization from the European Commission for LibmeldyTM, their ex vivo lentiviral gene therapy for MLD (the same disease described in Dr. Wolf’s paper). In clinical trials of Libmeldy, Orchard Therapeutics found that the gene therapy was effective in slowing progression of early-onset MLD in most cases. Treated patients were significantly more likely to preserve their ability to sit, stand and walk. What’s more, they typically did not experience the severe cognitive impairment expected in children with the disease. These are tremendous results, and I’m thrilled that their gene therapy has now been approved in Europe.
At AVROBIO, we are also advancing ex vivo lentiviral gene therapy for lysosomal disorders that require whole body treatment. We’re in the clinic with three investigational programs, for Fabry disease, Gaucher disease type 1 and cystinosis – all severe, progressive diseases that impact multiple systems from head to toe. We expect to enter the clinic for two of our “second wave” indications in the near future: Hunter syndrome, Pompe disease and Gaucher disease type 3. All of these disorders can have a destructive impact on cognitive and motor function. We are hopeful our whole-body approach to gene therapy may be able to prevent, halt or even reverse the relentless progression of these devastating symptoms.
We’ve learned a lot over the past few years about the power of ex vivo lentiviral gene therapy to enable treatments that reach head to toe, including the brain and spinal cord. I’m excited to be part of a team at the forefront of this field. All of us are driven by the potential to improve the lives of people with genetic disease – and day by day, I believe we’re making strong progress toward that goal.